Medical Interaction Guidelines for Dental Hygiene Treatment
Blood Pressure:
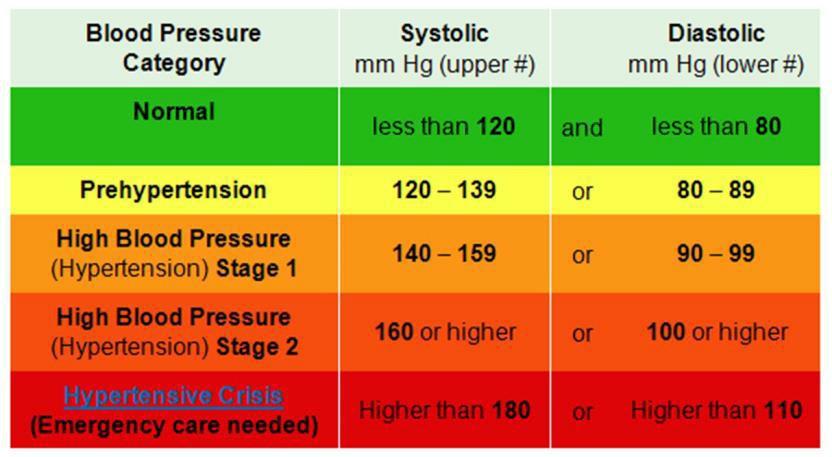
- 120-139 (systolic) over 80-89 (diastolic): Pre-hypertension
- 140-159 (systolic) over 90-99 (diastolic): Patients with this BP reading should be issued a medical consult at the completion of all the dental hygiene services.
- Pressure should be taken again 5 minutes later using a manual cuff to confirm the reading. Ask the patient to keep legs uncrossed.
- If multiple appointments are needed to finish dental hygiene services, the patient should be scheduled again within 2 weeks. If pressure remains elevated after three consecutive appointments, consult with patient’s physician or cardiologist before proceeding.
- Record all multiple BP readings, Pulse and Respiration on the consult along with any medications (and dosage) the patient is taking.
- Patient should be advised that the consult is to be returned to the school prior to scheduling their next recall appointment.
- Any local anesthesia concerns should be discussed with dental hygiene faculty and /or attending DDS.
- 160-179 (systolic) over 100- 109(diastolic): Patients with this BP may be seen for noninvasive procedures only without a medical consult.
- 180 and above (systolic) over 110 and above (diastolic): Patients who are stable/asymptomatic other than this BP reading require an immediate visit to the ER or that they see their physician immediately. No treatment is initiated. The patient is given a medical consult to have completed and returned before any treatment can take place. If the patient has any symptoms such as headache, nosebleed, etc., phone Campus Police at 711, and they will have an ambulance sent to the dental school.
- If patient’s BP drops under 50 diastolic, this constitutes a medical emergency. Always check your equipment before activating EMS if the patient is not symptomatic.
Coumadin/Warfarin and Other Blood Thinners:
All patients taking Coumadin MUST have a medical consult signed by a physician prior to receiving treatment. Consult should request Patient’s INR count. Multiple drug interactions should be carefully reviewed for possible emergencies due to their anticoagulation properties.
INR Guidelines
If the INR value is less than or equal to 2.5- 3.0 -- proceed
If it is higher than 3.0 – may not treat—medical consult needed
If the INR is unknown – must acquire a med consult
All patients on Coumadin must have a med consult annually.
Patients taking Plavix or other antiplatelet medication should send a Medical Consult to the patient’s physician post treatment indicating patient’s response to treatment (and what services were provided) and bleeding complications if any. PLEASE be sure to check patient charts prior to scheduling appointments so this can be taken care of BEFORE they report for their appointments. Document their current INR whenever possible.
Blood Disorders/HIV
Medical clearance must be obtained prior to treatment of any patient with an uncontrolled bleeding disorder or irregularities that would severely compromise the patient’s immune system. HIV Medical clearance and/or premed may be necessary if the current blood work shows any of the following. If you have any specific questions, please consult with the PLUS clinic. All lab values must be within a year of treatment at the Dental School.
| WBC: if under 2,000 will need antibiotics to treat |
Platelet count: must be at least 60,000 |
| Neutrophils: if < 500 need antibiotics to treat |
CD4: should be over 200 |
Total CD4+ count
Normal:
CD4+ cell counts in people who are not infected with HIV usually range from 600 to 1,500 cells per microliter.
Abnormal:
A CD4+ cell count greater than 350 but less than 500 cells/mcL means that the immune system is beginning to weaken.
A CD4+ cell count of fewer than 350 cells/mcL indicates a weak immune system and an increased risk for opportunistic infections.
A CD4+ cell count of fewer than 200 cells/mcL indicates acquired immunodeficiency syndrome (AIDS) and a high risk for opportunistic infections.
Source: http://www.webmd.com/hiv-aids/cd4-count
Patients may also report the Viral Load (VL) number:
What HIV Viral Load Test Results Mean
The HIV viral load test measures the number of HIV copies in a milliliter of blood.
- If the HIV viral load is high, HIV is reproducing and the disease may progress more quickly. A high HIV viral load is 50,000 to 100,000 copies. It can be as high as 1 million or more.
- If the HIV viral load is low, HIV may not be actively reproducing and the disease may progress more slowly. A low viral load is between 20 and 500 copies. However, what you want is an undetectable viral load
- If the HIV viral load can't be detected, this does not mean it is cured. The level of HIV virus may be so low that the test can't pick it up. A more sensitive test may be able to detect it. It's important to also know that the HIV viral load test does not measure HIV in other parts of the body where HIV may be present. Only about 2% of HIV is in the blood. For most patients, the goal of treatment is to reach an undetectable viral load, which is currently defined as less than 20 copies.
Remember: Even if the HIV viral load is undetectable, HIV positive patients can still infect others.
Source: http://www.webmd.com/hiv-aids
Dialysis and Diabetes
Kidney Dialysis:
Medical consult should be given prior to receiving treatment requesting:
- Need for premedication for invasive procedures (ie: deep scaling and root planning)
- Request a Complete Blood Count (CBC) that may identify potential bleeding problems and reduction in healing.
*Dental appointments should be NOT made on the same day of dialysis. Blood pressure should be taken on the arm without the hemodialysis shunt.
Diabetes Blood Glucose Levels:
Patients diagnosed with Diabetes should have a blood/glucose level of <180 if they have eaten/ <130 fasting to receive treatment in the dental school. HbA1C should be reported by the patient and <7 is considered controlled. For readings >140-250 the patient can be seen for non-invasive care but will require a med consult for future appointments. Any patient with a reading over 250 cannot be seen for treatment that day. If a reading is taken and it falls < 70 the patient can be given juice. If you have any reason to believe that the patient is not well controlled, have the nurse assess the patient.
| Target Blood Glucose Levels in People Who Have Diabetes |
| Before meals |
70 to 130 mg/dL |
| 1 to 2 hours after the start of a meal |
below 180 mg/dL |
Source: American Diabetes Association. Standards of Medical Care in Diabetes—2008. Diabetes Care. 2008; 31:S12–S54.
Ideally, patients should be scheduled in the morning when their insulin is working in balance with the foods they have eaten. Since dental hygiene appointments at the dental school expand over several hours, the diabetic patient should be monitor closely for
Signs of Hypoglycemia:
Hunger/Weakness
Trembling/Anxiety
Sweating
Tachycardia Confusion
Monitor the patient closely for any of these signs. Keeping appointment short may be best for the patient. If patient exhibits signs of confusion:
Give patient some form of sugar for the (conscious victim) ie: Juice, hard candy
OR- instruct nearby dh student to get Emergency Cart with sucrose tube – place under patient’s tongue. Report to faculty and nurse.
Follow Emergency Protocols for the unconscious patient.
Recent heart attack or stroke
http://www.colgate.com/app/Colgate/US/OC/Information/OralHealthBasics/MedCondOralHealth/HeartDiseaseOralHealth/Cardiovascular.cvsp
Patients who have had a stroke or heart attack cannot receive dental treatment for 6 months after the vascular event and will need medical consult prior to treatment just following that.
See additional cardiac guidelines under IE and premedication.
Pregnancy (from UMB School manual 04-05):
- Each pregnant patient must be individually evaluated to establish the appropriate extent of dental treatment. A medical consult is appropriate prior to the provision of definitive treatment. Please review guidelines regarding the exposure of radiographs in the pregnant patient.
- Emergency dental care for pregnant patients will be provided on an individual basis following an assessment of the medical status and the risk associated with the dental treatment.
- This is outdated. Pregnant patients may be seen throughout their pregnancy.
GP Directors should be informed of any potential medical complication
If after consulting the GP manager there is still some question, call the patient’s physician for clearance and have them fax copy to the reception desk.
| 2nd Floor 410-706-6280 |
3rd Floor 410-706-6279 |
School nurse fax 410-706-6030 |
Infective Endocarditis Prevention Guidelines, UMB Dental School COB
The AHA/ADA recommends that most patients no longer need short-term antibiotics as a preventive measure before their dental treatment. Only those patients with the highest risk should receive prophylaxis.
The following highest risk individuals should receive IE prophylaxis:
- Artificial heart valves
- A history of infective endocarditis
- Certain specific, heart conditions, including
- unrepaired or incompletely repaired cyanotic congenital heart disease, including those with palliative shunts and conduits
- a completely repaired congenital heart defect with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first six months after the procedure
- any repaired congenital heart defect with residual defect at the site or adjacent to the site of a prosthetic patch or a prosthetic device
- An individual with cardiac transplant that develops a problem in a heart valve.
The guidelines recommend that except for the highest risk patients listed above, patients who have taken prophylactic antibiotics routinely in the past no longer need them.
This includes patients with:
- mitral valve prolapse
- rheumatic heart disease
- bicuspid valve disease
- calcified aortic stenosis
- congenital heart conditions such as ventricular septal defect, atrial septal defect and hypertrophic cardiomyopathy.
The drug regimens have remained unchanged.
For those patients who are taking an antibiotic for another condition the patient must take another class of antibiotic for pre-medication prior to their dental appointment.
It is the responsibility of every clinician to adhere to the standard of care, which is, in this case, the new AHA Guidelines.
American Heart Associate Guidelines for the Prevention of Infective Endocarditis (IE)
Box 2. Primary Reasons for Revision of the IE Prophylaxis Guidelines.
IE is much more likely to result from frequent exposure to random bacteremias associated with
Box 3. Cardiac Conditions Associated with the Highest Risk of Adverse Outcome from Endocarditis for which Prophylaxis for Dental Procedures is Reasonable.
- Prosthetic Cardiac Valve or prosthetic material used for cardiac valve repair
* Except for the conditions listed above, antibiotic
┼Prophylaxis is reasonable because endothelialization
Box 4. Dental Procedures for which Endocarditis Prophylaxis is Reasonable for Patients in Box 3.
All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa*
*The following procedures and events do not need prophylaxis: routine
Table 2. Regimens for a Dental Procedure.
|
Regimen: Single dose 30-60 minutes before procedure |
| Situation |
Agent |
Adults |
Children |
| Oral |
Amoxicillin |
2 g |
50 mg/kg |
| Unable to take oral medication |
Ampicillin
OR
Cefazolin or Cephtriaxone |
2 g IM* or IV┼
OR
1 g IM or IV |
50 mg/kg IM or IV |
| Allergic to penicillins or ampicillin – oral |
Cephalexin╪§
OR
Clindamycin
OR
Azithromycin or Clarithromycin |
2 g
OR
600 mg
OR
500 mg |
50 mg/kg
OR
20 mg/kg
OR
15 mg/kg |
| Allergic to penicillins or ampicillin – unable to take oral medication |
Cefazolin or Cephtriaxone§
OR
Clindamycin |
1 g IM or IV
OR
600 mg IM or IV |
50 mg/kg IM or IV
OR
20 mg/kg IM or IV |
*IM: intramuscular, ┼IV: intravenous
╪Or other first- or second-generation oral cephalosporin in equivalent adult or pediatric dosage.
§Cephalosporins should not be used in a person with a history of anaphylaxis, angioedema, or urticaria with penicillins or ampicillin.
The complete guidelines as they relate to dentistry are published in The Journal of the American Dental Association 2008; 139(1): Special Supplement.
Modified from: Preventing Infective Endocarditis, J Am Dent Assoc 2008: 139(1) Special Supplement: 7s, 17S, 18S, 20S.
Total Joint Replacement:
Total Joint Replacement http://www.ada.org/en/member-center/oral-health- topics/antibiotic-prophylaxis#replace
In 2012, the American Dental Association and the American Academy of Orthopaedic Surgeons (AAOS) released the first co-developed evidence-based guideline on the Prevention of Orthopedic Implant Infection in Patients Undergoing Dental Procedures. The clinical practice guideline, with three recommendations, is based on a systematic review of the literature. The review found no direct evidence that dental procedures cause orthopedic implant infections.
The following is a summary of the recommendations of the AAOS-ADA clinical practice guideline, Prevention of Orthopedic Implant Infection in Patients Undergoing Dental Procedures. This summary does not contain rationales that explain how and why these recommendations were developed, nor does it contain the evidence supporting these recommendations. All readers of this summary are strongly urged to consult the full guideline and evidence report for this information (see link below). We are confident that those who read the full guideline and evidence report will see that the recommendations were developed using systematic evidence-based processes designed to combat bias, enhance transparency, and promote reproducibility.
This summary of recommendations is not intended to stand alone. Treatment decisions should be made in light of all circumstances presented by the patient. Treatments and procedures applicable to the individual patient rely on mutual communication between patient, physician, dentist and other healthcare practitioners.
The Guideline Recommendations:
- The practitioner might consider discontinuing the practice of routinely prescribing prophylactic antibiotics for patients with hip and knee prosthetic joint implants undergoing dental procedures.
Strength of Recommendation: Limited
A Limited Recommendation means the quality of the supporting evidence that exists is unconvincing, or that well-conducted studies show little clear advantage to one approach versus another.
Practitioners should be cautious in deciding whether to follow a recommendation classified as Limited, and should exercise judgment and be alert to emerging publications that report evidence. Patient preference should have a substantial influencing role.
- We are unable to recommend for or against the use of topical oral antimicrobials in patients with prosthetic joint implants or other orthopedic implants undergoing dental procedures.
Strength of Recommendation: Inconclusive
An Inconclusive Recommendation means that there is a lack of compelling evidence resulting in an unclear balance between benefits and potential harm.
Practitioners should feel little constraint in deciding whether to follow a recommendation labeled as Inconclusive and should exercise judgment and be alert to future publications that clarify existing evidence for determining balance of benefits versus potential harm. Patient preference should have a substantial influencing role.
- In the absence of reliable evidence linking poor oral health to prosthetic joint infection, it is the opinion of the work group that patients with prosthetic joint implants or other orthopedic implants maintain appropriate oral hygiene.
Strength of Recommendation: Consensus
A Consensus Recommendation means that expert opinion supports the guideline recommendation even though there is no available empirical evidence that meets the inclusion criteria.
Practitioners should be flexible in deciding whether to follow a recommendation classified as Consensus, although they may set boundaries on alternatives. Patient preference should have a substantial influencing role.
If you have any questions about these recommendations, please contact the ADA Division of Science via email. ADA members may also use the Association’s toll-free number and ask for x2878.
Additional Resources for ADA/AAOS Guidelines
- Full Guideline: Prevention of Orthopedic Implant Infection in Patients Undergoing Dental Procedures (PDF)
- Executive Summary: Prevention of Orthopedic Implant Infection in Patients Undergoing Dental Procedures (PDF)